Tick species that transmit Rocky Mountain spotted fever: Rocky mountain wood tick (Dermacentor andersoni), American dog tick (Dermacentor variabilis), Brown dog tick (Rhipicephalus sanguineus).
What is Rocky Mountain Spotted Fever?
Rocky Mountain spotted fever (RMSF) is the most serious tick-borne disease in the United States and is caused by Rickettsia rickettsii, a type of bacteria known as rickettsia. These bacteria are transmitted to humans by the bite of certain hard ticks. The two most important species of ticks that can transmit R. rickettsii in the United States are Dermacentor variabilis (the American dog tick) and Dermacentor andersoni (Rocky Mountain wood tick). A third species, Rhipicephalus sanguineus (brown dog tick) has been implicated as a vector. Dogs are susceptible to RMSF, and sometimes household members of infected dogs may also be at risk for acquiring the disease. In countries south of the United States, the cayenne tick (Amblyomma cajennense) has also been shown to act as a vector of RMSF.
More recently another rickettsie has been identified as the cause of a spotted fever-like disease. Theis species, called Rickettsia parkeri, was first identified more than 60 years ago in Amblyomma maculatum ticks (Gulf coast ticks). Confirmation of R. parkeri as a causative agent of human disease occurred in 2002 when serological (blood) tests, immunohistochemical staining, cell culture isolation and other molecular tests positively verified infection in a patient.
The classic symptoms of RMSF include fever and a spotted (petechial) rash, although they are not always present. RMSF can be a fatal disease and patients often require hospitalization. Severe illness is seen more often in patients who delay seeking care from a physician because such patients do not receive antibiotic treatment as soon as they should. RMSF is considered an acute infection and infection with Rickettsia rickettsii is thought to provide long-lasting immunity against re-infection, however this should not deter those who feel they suffer symptoms from seeking care. RMSF is typically treated with a course of tetracycline antibiotics (CDC).
Where is Rocky Mountain Spotted Fever Prevalent?
Although first recognized in the late 19th century in the Rocky Mountain region, by 1930s this disease was found to be present in the eastern portion of the country as well. The wood tick (Dermacentor andersoni), one of the main tick vectors is found in the Rocky Mountain states and southwestern Canada. The second major vector is the American dog tick (Dermacentor variabilis). This tick is distributed east of the Rocky Mountains and in some regions along the Pacific Coast. The cayenne tick (Amblyomma cajennense) is found in South and Central America; however its range also extends into some southern states including Texas. The most recently implicated vector of R. parkeri is the lone star tick (Amblyomma americanum). It is found in southern states as well as along the East coast up to Maine.
There has been a marked drop in incidence of RMSF in the Rocky Mountain States since the 1940s. Today over half of the cases of RMSF occur in South Atlantic states (Delaware through Florida). Rocky Mountain spotted fever is a seasonal disease with the majority of cases occurring between the months of April and September. Clustered cases of RMSF have occurred among families in states including Kentucky, Arizona and Oklahoma. Rocky Mountain spotted fever is a nationally notifiable disease to the CDC, and cases are reported via two national surveillance systems, standardized case report forms and the National Electronic Telecommunications System for Surveillance (NETSS). Cases are considered confirmed or probable based on results of laboratory tests. Over the last fifty years approximately 250 to 1200 cases have been reported annually.
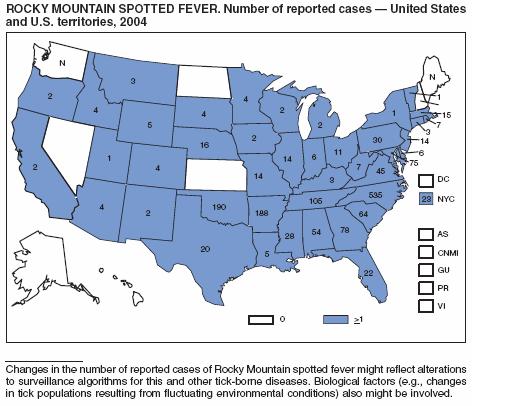
Image obtained from CDC MMWR Report
Symptoms
Symptoms of Rocky Mountain spotted fever usually appear 2 to 14 days (average of 7 days) after being bitten by the infected tick. Fever is often the first symptom experienced by patients. The classic triad of fever, rash and tick bite is present among many but not all cases at the initial visit to the physician. Nausea, vomiting, severe headache, muscle pain and lack of appetite are also sometimes reported by patients in the early stage of disease. Other clinical symptoms include abnormal platelet count (thrombocytopenia), elevated liver enzymes, and electrolyte abnormalities. The initial rash tends to appear 2 or 3 days after onset of the illness as small pink non-itchy spots (macules) on the skin that later become the characteristic spotted red rash (petechiae). The rash is most often found on ankles and wrists and then appears on trunk, palms and soles. The characteristic petechial rash occurs in only 35 to 60 % of patients, and as many as 10 to 15% of patients may never develop a rash. Other late stage symptoms associated with RMSF include abdominal pain, joint pain, and diarrhea.
Late Petechial Rash on Forearm of RMSF Patient

Symptoms of the spotted fever like disease caused by the most recently implicated rickettsia, R. parkeri, are very similar to those caused by R. rickettsii. However, while lesions (called eschars) at the site of the tick bite rarely occur in R. rickettsii-associated RMSF, they do occur in infections caused by R. parkeri.
Diagnosis
Clinical diagnosis of RMSF is based on serological tests including detection of antibody titers via IFA, detection of the bacterial agent via culture or immunohistochemical staining of biopsies, and by detection of bacterial DNA in a clinical specimen via PCR. However, treatment decisions should not be delayed while waiting for confirmation with laboratory results. Patients with a relevant history and symptomology should be treated with the appropriate antibiotic regimen immediately.
Since the R. rickettsii and R. parkeri bacterial species are so closely related, cross-reactivity between these two agents may make it difficult to distinguish between them using less specific serological or immunohistochemical assays.
Treatment
Upon suspicion of Rocky Mountain spotted fever, treatment should begin immediately. Delay of treatment has been associated with fatal outcomes. Treatment with tetracycline or chloramphenicol antibiotics can be used to treat RMSF. Doxycycline (a tetrycycline) antibiotic is the treatment of choice for both adults and children. However doxycycline is not recommended for use by pregnant women. Current recommendations from the Centers for Disease Control and Prevention (CDC) include doxycycline therapy for 5 to 10 days. Complicated disease cases may require longer treatment. Patients usually see an improvement in fever 24 to 72 hours after starting antibiotics.